

Capturing clinically relevant genomic insights
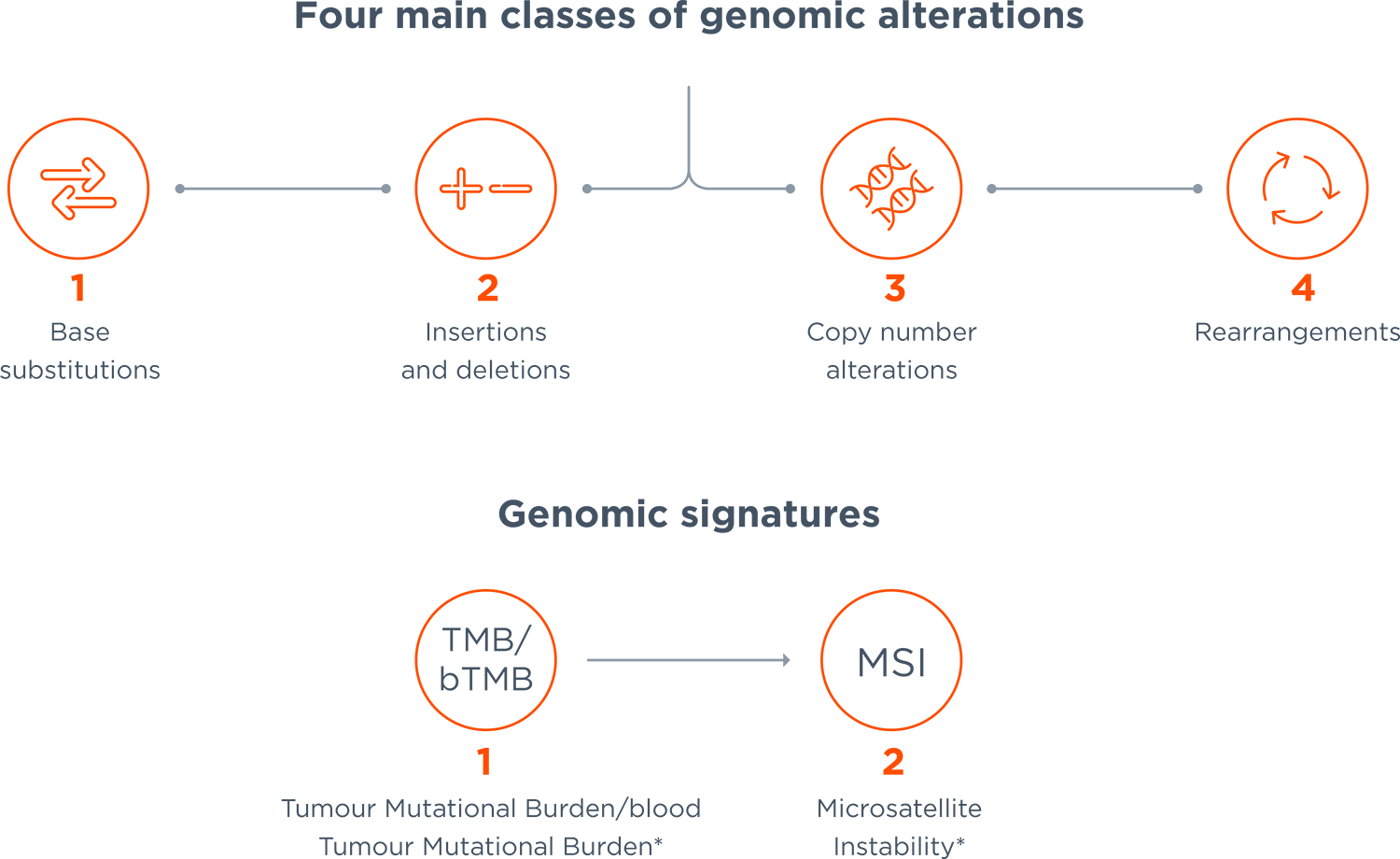
There are four main classes of genomic alterations: base substitutions, insertions or deletions, copy number alterations and gene rearrangements. But are current diagnostic approaches up to the task of identifying them all? Single biomarker tests, using common diagnostic techniques such as PCR/IHC/FISH, and multigene hotspot NGS tests risk missing genomic alterations that may be critical to patients’ treatment plans.4,11–13
Furthermore, complex pan-tumour genomic signatures, such as Tumour Mutational Burden (TMB), blood Tumour Mutational Burden (bTMB) and Microsatellite Instability (MSI), may provide further valuable insights to help personalise treatment plans. MSI informs eligibility for immunotherapy and is a cancer guideline-recommended signature.14–18 TMB and bTMB are exploratory genomic signatures that inform eligibility for immunotherapies independently of PD-L1 expression.19–24 Comprehensive genomic profiling is the only viable routine clinical option for measuring TMB and bTMB.19–22
*TMB reported by FoundationOne CDx and FoundationOne Heme. bTMB reported by FoundationOne Liquid CDx. MSI reported by FoundationOne CDx and FoundationOne Heme, MSI-H reported by FoundationOne Liquid CDx.
Date of item: January 2022. M-IE-00000628
References
- Rozenblum AB et al. J Thorac Oncol 2017; 12: 258–268.
- Schwaederle M, Kurzrock R. Oncoscience 2015; 2: 779–780.
- Mansinho A et al. Expert Rev Anticancer Ther 2017; 17: 563–565.
- Frampton GM et al. Nat Biotechnol 2013; 31: 1023–1031.
- Drilon A et al. Clin Cancer Res 2015; 21: 3631–3639.
- Hirsch FR et al. Lancet 2016; 388: 1012–1024.
- Baumgart M. Am J Hematol Oncol 2015; 11: 10–13.
- Chakravarty D et al. JCO Precis Oncol 2017; doi: 10.1200/PO.17.00011.
- Global Oncology Trends Report 2018. Report by IQVIA Institute for Human Data Science. Available at: https://www.iqvia.com/-/media/iqvia/pdfs/institute-reports/global-oncology-trends-2019.pdf (Accessed August 2021).
- Gagan J, Van Allen EM. Genome Med 2015; 7: 80.
- Schrock AB et al. Clin Cancer Res 2016; 22: 3281–3285.
- Rankin A et al. Oncologist 2016; 21: 1306–1314.
- Suh JH et al. Oncologist 2016; 21: 684–691.
- Zhao P et al. J Hematol Oncol 2019; 12: 54.
- Abida W et al. JAMA Oncol 2019; 5: 471–478.
- Kok M et al. ESMO Open 2019; 4(Suppl 2): e000511.
- NCCN Clinical Practice Guidelines in Oncology. Prostate Cancer. Version 2.2020, May 2020. Available at: https://www.nccn.org/guidelines (Accessed August 2020).
- FDA approves pembrolizumab for first-line treatment of MSI-H/dMMR colorectal cancer. Available at: www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-pembrolizumab-first-line-treatment-msi-hdmmr-colorectal-cancer (Accessed August 2021).
- FDA approves pembrolizumab for adults and children with TMB-H solid tumors, 2020. Available at: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-pembrolizumab-adults-and-children-tmb-h-solid-tumors (Accessed August 2021).
- Gandara DR et al. Nat Med 2018; 24: 1441–1448.
- Yarchoan M et al. JCI Insight 2019; 4: e126908.
- Marabelle A et al. Ann Oncol. 2019;30(suppl_5):v475-v532.
- Socinski M. Ann Oncol 2019; 30(suppl_5): v851–v934.
- Khagi Y et al. Clin Cancer Res 2017; 23: 5729–5736.
- NCCN Clinical Practice Guidelines in Oncology. Non-Small Cell Lung Cancer. Version 6.2020, June 2020. Available at: https://www.nccn.org/guidelines (Accessed August 2020).
- Kalemkerian GP et al. J Clin Oncol 2018; 36: 911–919.
- Lindeman NI et al. J Mol Diagn 2018; 20: 129–159.